A mild form of cholera, sometimes known as British or English Cholera, infantile diarrhoea, summer diarrhoea or epidemic gastroenteritis had long been recognised in Britain but in the early 1830s a far more deadly form made its way to our shores.
Originating in India, it acquired the names ‘Asiatic Cholera’ or ‘Cholera Morbus’ to distinguish it from the localised form. Asiatic Cholera is now known to be caused by an endotoxin produced by the bacterium Vibrio cholerae. Highly infectious with a high mortality rate, it is usually spread by contaminated food and water caused by unsanitary conditions. Symptoms include diarrhoea, persistent vomiting, severe cramps, muscular weakness, dehydration and circulatory collapse. This latter stage, resulting in the patient taking on a blue tinge, led to another name – the Blue Plague.
It was first spotted in Goa, India in 1817, thereafter it was carried through the trade routes, spreading first through Southeast Asia and the Middle East, then westwards to Russia and Europe reaching Vienna and Berlin in August 1831. Despite attempts to prevent its spread to Britain by quarantining ships arriving from continent, the first recognised case of Asiatic Cholera in Britain was recorded in Sunderland in October 1831. By the end of the outbreak in 1832, it is estimated to have killed 32,000 people in Britain alone.
Outbreaks of 1848/1849 and 1853/1854
The social reformer Edwin Chadwick’s (1800-1890) publication
‘The Sanitary Conditions of the Labouring Population’ (1842) made the link between disease and poor sanitary conditions but nothing changed. However the second cholera epidemic of 1848 and 1849, which killed 62,000 Britons (13,565 in London), led to the Public Health Act of 1848 and the establishment of the general Board of Health, for which Chadwick became the first director.
|
Extract of a letter from Richard Owen to Roderick Murchison, [1848]. Archive ref: LDGSL/838/O/7/13
Best known for his palaeontological work, Society Fellow Richard Owen (1804-1892) was also involved in Sanitary Reform notably reporting to the Royal Commission on the Health of Towns in 1845.
This letter references that he has been summoned by the public health reforming MP Lord Morpeth [George William Frederick Howard (1802-1864)] and Edwin Chadwick to help with the Cholera outbreak which has reached Hull and London. Archive ref: LDGSL/838/O/7/13. Click to enlarge.
|
On 31st August 1854 an outbreak of cholera was first detected in Broad Street, London. Within ten days, it had killed over 500 people. The physician John Snow (1813-1858) had theorised that cholera was a waterborne disease during the previous epidemic of 1849, when he noted that the areas supplied by the Lambeth and Southwark & Vauxhall water companies were hit particularly hard. Snow therefore looked to the local water supply. Mapping the locality of the deaths, his analysis showed that they were in the vicinity of the Broad Street water pump. The well which supplied the water had been infected by sewage which had leaked from a nearby cesspit. The pump’s handle was removed and the infection rate (which was falling anyway) stopped. London’s 1854 cholera epidemic killed 10,684 of its inhabitants.
Outbreak of 1866
|
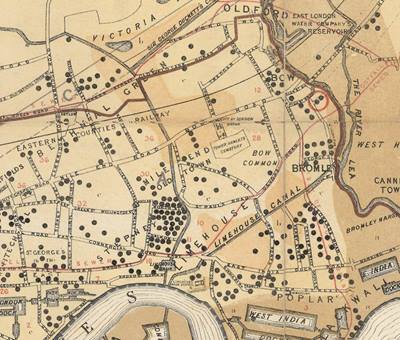
Extract from ‘[Geological] Map showing the distribution of Cholera in London and its Environs from June 27th to July 21st 1866’, (1866). GSL Library collection. The two black dots encircled in red indicate a married couple who were the first confirmed cases of the 1866 epidemic. The Old Ford reservoir can be seen at the top.
|
In 1866 the country suffered another outbreak of Asiatic cholera. The first death is thought to have been a sailor from Rotterdam travelling to Bristol who died on the 28th April. By May the port cities in the north east and west of England reported numerous cases amongst German and Dutch emigrants who intended to travel to New York from Liverpool. The southern port cities reported further cases in June.
Deaths from British cholera or choleraic diarrhoea were common amongst London’s poor due to the living conditions and lack of clean water supply. This disguised to a certain extent the detection of the more severe form when cases began to appear in June.
From July, the nature of the epidemic became clear and case numbers exploded. The week ending the 14th July saw 32 deaths registered, but by the 4th August 1,053 people died within the preceding seven days. After 23 weeks from the outbreak of the epidemic, there were 5,548 deaths recorded in London, 3,909 were of people living in the East End.
The creation of the geological map above was influenced by the German chemist and public health official Max von Pettenkofer’s (1818-1901) now outdated theory that cholera epidemics would only happen under particular circumstances. It relied on three elements combining: the standard of health of the individual; the environmental/meteoric conditions; and the disease ‘fermenting’ in the groundwater of low level areas.

|
| William Whitaker, FGS [1865-1877]. Archive ref: GSL/POR/44/03-04 |
The medical officer J N Radcliffe marked the distribution of cholera deaths which occurred between 27th June and 21st July 1866 on a geological map to analyse whether the localised geological and topographical conditions had any bearing on the infection. Pettenkoffer was indisposed so Radcliffe called upon the services of Society Fellow William Whitaker (1836-1925) to help him. The geology on the map is taken from Robert Mylne’s ‘Topographical [and Geological] Map of London and its Environs’ (1851). The map demonstrates that neither the geology nor the elevation/depression of the land had any bearing as the most affected places shared similar conditions to those which were hardly touched.
Instead it shows that the areas with the highest mortality rate shared a common water supply from the Old Ford reservoir operated by the East London Waterworks Company. Whilst the intake source on the River Lea was above the outlet for one of the main sewers for London, the tidal nature of the Thames meant it flowed back up and contaminated the reservoir. Additionally the only treatment (filtering) was obstructed during the summer months by thick, slimy growths of algae.
In 1883, the German microbiologist Robert Koch (1843-1910) discovered the bacterium which caused cholera. Pettenkofer, in a bid to prove that his tripartite idea was still valid, drank a sample containing Vibrio cholerae supplied by Koch in 1892. He suffered symptoms for around a week afterwards.
<<Back to main page
Next: Artesian Wells>>